Los Angeles County is fast becoming the epicenter of the pandemic in the United States. ⦿ Multi-generational households remain the principal pathway for coronavirus transmission. ⦿ Community health centers will be critical to getting through the hard winter to come.
Go Where the Virus Is.
The map below captures the main message of this article: Go where the virus is.
The rose-shaded areas are the Los Angeles County communities where the per-capita incidence of newly confirmed COVID-19 cases grew the fastest during the three weeks ending December 17. While these communities together contain half of the population of the county, their residents now make up nearly two-thirds of all newly diagnosed infections.
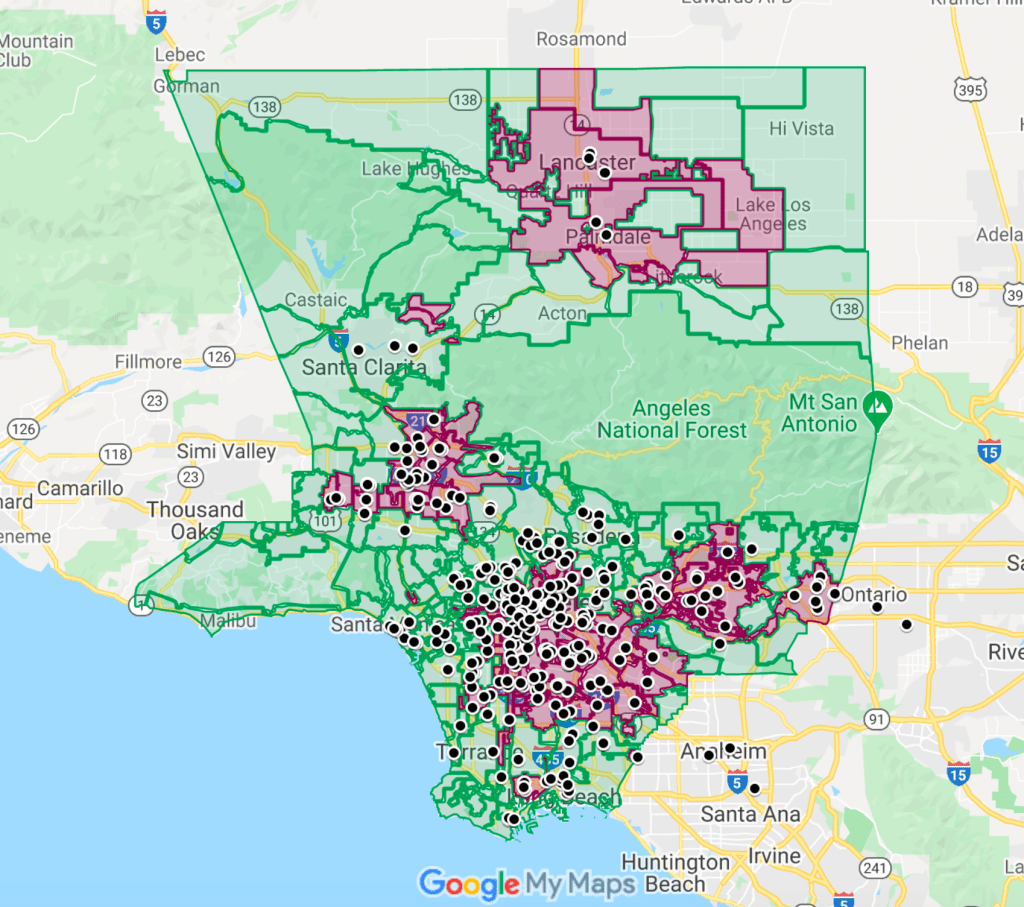
The black circles mark the locations of 353 member clinics of the Community Clinic Association of Los Angeles County (CCALAC). These community health centers are uniquely situated to confront the epidemic surge that is already overwhelming the county’s acute-care hospital capacity.
Actually, these health centers don’t have to move an inch to go where the virus is. They’re already there.
The Winter Surge Has Arrived.
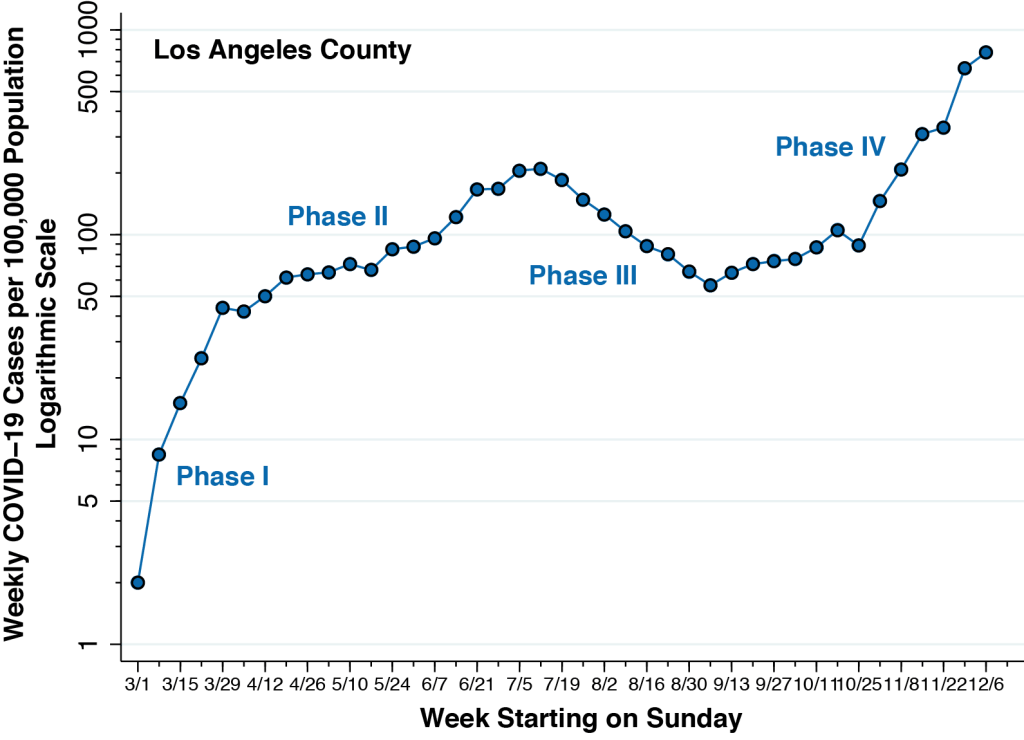
Figure 2 below updates the weekly incidence of newly diagnosed COVID-19 cases in Los Angeles County, running from the week starting March 1 through the week starting December 6, 2020. When we last studied the Los Angeles County epidemic, we could see the emergence of a fourth phase during September. Now, the Phase IV surge is obvious. The incidence of newly confirmed COVID-19 cases per 100,000 during the week of December 6 is nearly four-fold the peak incidence seen during the week of July 12.
Los Angeles Mayor Eric Garcetti’s recent stay-at-home order may indeed retard the growth of new cases in the weeks to come. But it will not change the fundamentals of SARS-CoV-2 transmission. Herd immunity from mass vaccination is likely to be several months off.
There is, to put it graphically, no easy way to extinguish the virus-flames that will rage during the winter months to come.
Multi-Generational Household Transmission
Figure 3 compares two maps of Los Angeles County. Each map is broken down into countywide statistical areas (CSAs), a hybrid geographic classification of independent municipalities such as the City of Beverly Hills, neighborhoods of Los Angeles such as Hollywood, and unincorporated places such as Hacienda Heights.

On the left, the CSAs are color-coded according to the number of newly confirmed COVID-19 cases per 100,000 recorded during November 27 – December 17, 2000. On the right, the same CSAs are coded according to the proportion of households that we’ve identified as at risk for multi-generational transmission. As explained in this detailed report (which, for those who care, remains under peer review), we classified a household as at risk for multi-generational transmission if it had at least four persons, at least one person 18–34 years of age and another person was at least 50 years of age.
The two maps in Figure 3 show striking a concordance. Those communities with the highest prevalence of at-risk households, as depicted on the right, had the highest incidence of recent COVID-19 infection, as shown on the left. While we’ve previously noted the concordance with cumulative incidence through September 19 and through November 26, the comparison here is with the number of newly incident cases during the last three weeks of Phase IV.
In short, transmission within multi-generational households continues to dominate the Los Angeles County pandemic.
For those who don’t see the straight visual comparison of two maps as convincing, the technical section below offers a more rigorous demonstration.
The Data Fit With What We See on the Battlefield.
There isn’t the remotest doubt at this juncture that the numbers of confirmed cases reported through voluntary testing substantially understate the actual numbers of incident SARS-CoV-2 infections. Asymptomatic persons, we now know, are responsible for at least 40-45 percent of cases and play a dominant role in disease transmission. Still, the official public statistics fit with what we’re now seeing, as they say, en el campo de batalla.
The clinical histories, one by one, are remarkably the same. One person – usually an asymptomatic or pre-symptomatic young adult – has unknowingly imported the infection into the household. By the time the first member of the household displays any symptoms, all of them – children, adolescents, parents, aunts, uncles, grandparents – have already been infected.
In one household, a woman in her 40’s, having just come down with body aches, fever, and loss of smell, isolated her daughter and her mother in one bedroom and her son and father in another bedroom. The 23-year-old son, who turned out to be patient zero in this particular family, infected his 83-year-old grandfather roommate, who naturally became the focus of considerable clinical attention. (I have intentionally altered the ages of family members.)
The supreme irony of this and so many other cases is that nearly everyone in the household was taking special care to avoid contagion. The parents would make limited trips to the market, always wearing masks. Many grandparents would never go out at all.
Are the young adults who unintentionally import their infections into their multi-generational families simply being careless or ignorant? Not exactly. A young adult who turned out to be patient zero in his own family always wore his mask at work. When he went jogging with his buddies after work, they kept their distance. After one run, they all went for some cold refreshments.
One of the friends ordered hot tea. He just had allergies, he said.
The Super-Spreader Fallacy
It has become fashionable to talk about super-spreader events as the key driver of the current epidemic. It certainly raises eyebrows when we read a report that hundreds of people got infected at an assisted living facility, detention center, sports arena, food processing plant, or wedding reception.
But that can’t possibly be the dynamic underlying the emergence of Los Angeles as the new North American epicenter. Los Angeles does not have a monopoly on wedding receptions, scientific meetings, political rallies, or church choir practices.
It’s all in the math. Multi-generational households at risk for viral transmission make up 13.8 percent of all households in Los Angeles County. With an estimated 3.3 million households in the county, we’re talking about 455,000 multi-generation households where an asymptomatic or mild SARS-CoV-2 infection in a younger household member would put older household members at significant risk.
Let’s round off the size of the average multi-generation household to just 5 members. During the last three weeks, well over 1 percent of these households were infected. And let’s say the typical super-spreader event generates 100 cases, at least during the first round of transmission. The rest is arithmetic.
During the past three weeks, propagation of the virus through multi-generational households in Los Angeles County has been the equivalent of 200 so-called super-spreader events.
Community Health Centers Are the Key.
The Google Map below is a navigable version of the screenshot shown at the beginning of this article. It is worth repeating that the hot spots with the highest incidence of new infection are precisely the places where multi-generational families are most prevalent.
What’s more, the members of those multi-generational families at highest risk for transmission are, by and large, already patients of nearby community health centers.
Here Are Some of the Things Health Centers Could Do.
Here is an abbreviated list of the things that these community health centers could do – if only they were immediately given adequate resources.
- Community health centers need to be equipped to perform high-volume SARS-CoV-2 testing of their patients, with a focus on bringing in all household members at the same time.
It is widely acknowledged that testing needs to be more proactive. We can’t continue to sit back and wait for symptomatic people to come through the door. Workplaces and educational institutions have engaged in routine testing of asymptomatic people. Community health centers need to be the next locus of routine testing. Health centers know who are their high-risk patients. They are ideally positioned to bring in the entire families of these high-risk patients for routine testing.
- Community health centers need to be equipped with telemedicine technology, so that providers can rapidly respond to patients’ inquiries and concerns.
Surveys give us only an incomplete picture of the public’s knowledge of such basic issues as how COVID-19 is spread. The plain fact is that patients have an abundance of unanswered questions that apply to their specific circumstances.
Intelligent, useful answers to these questions require detailed knowledge of the incubation period of the virus, the time profile of viral shedding before and after symptoms appear, the likelihood of false-positive or false-negative tests, and the emergence of serious complications in the second critical week . Meaningful answers require clinical knowledge of whether COVID-19 can cause diarrhea, earache, body rashes, back pain. and anxiety due to a low oxygen level. Healthcare providers at community health centers are ideally positioned to answer these questions.
- Healthcare providers at community health centers are uniquely positioned to respond rapidly to patients who are at risk of deterioration.
If any reader has the remotest doubt where people in the United States turn when they feel really sick from COVID-19, here is the answer. They call 911.
And this is by no means an abuse of the public safety system. In a December 16 news release announcing that Los Angeles County now had more than 5,000 COVID-19 hospitalizations, the Department of Public Health stated in plain English: “If you are having difficulty breathing, go to an emergency room or call 911.” A December 22 news release announcing another 1,000 COVID-19-related deaths in the past two weeks stated in plain Spanish: “Si tiene dificultad para respirar, vaya a la sala de emergencias o llame al 911.”
Healthcare providers in community health centers are ideally positioned to address patients’ concerns. Who else is going to tell a COVID-19-stricken patient who can hardly eat anything whether she should still take her blood pressure or her diabetes pills? Who else is going to intelligently advise a patient when chest tightness becomes so severe that it’s time to go to the ER? The Department of Public Health has urged providers: “Do not send patients to emergency departments unless absolutely medically necessary.” Physicians, nurse practitioners, physicians’ assistants, and nurses know their patients. They can respond to the challenge if given the resources to do so.
- Community health centers could distribute pulse oximeters to their patients and instruct them on their use.
The pulse oximeter is now widely acknowledged as a critical tool in the outpatient evaluation of a patient acutely ill with COVID-19. Community health centers are ideally situated to distribute these devices to patients most in need. New York City is distributing oximeters to healthcare providers, and Los Angeles County health centers should get them, too. In abundance.
- Community health centers are well situated to provide timely outpatient treatment to high-risk COVID-19 patients.
There is growing evidence that monoclonal antibody infusions need to be given as early as possible to high-risk patients during the initial viremic phase of their illness. Recent controlled trials suggest that these medications may be ineffective if we wait until the patient is so ill as to need hospitalization. The same may be true for the antiviral drug remdesivir.
We need to identify high-risk patients at the onset of symptoms and establish outpatient facilities where trained personnel can administer these therapies. When it comes to Los Angeles County, community health centers could serve as the ideal locus for this new model of care. It is not difficult to imagine a health center-based nurse administering an infusion to a 70-year-old diabetic with a history heart and kidney problems within a couple of days of symptoms.
What About Social Distancing Measures?
How does this fit in with the now-enormous literature on the effectiveness of the social distancing measures? No one disputes that a great many of the emergency measures enacted by governments worldwide have substantially reduced the propagation of the virus. But the time has come to realize that these now-conventional measures – stay-at-home orders, closures of bars, restaurants, gyms, hair salons, movie theaters, restrictions on large gatherings – are no longer enough. And what’s worse, their enforcement may represent a misallocation of limited resources.
Los Angeles County authorities need to start thinking beyond their standard public health toolbox. They need to adapt their policies to the unique facts on the ground.
If public authorities in Los Angeles County diverted substantial additional resources to community health centers, we’d still have a real chance at putting out the virus-flames.
Technical Details on Multi-Generational Household Transmission
Figure 4 offers another way visualize the critical role of intra-household transmission in the Los Angeles epidemic. We’ve graphed the number of newly recorded cases per 100,000 during November 17 – December 17 against the corresponding number of new COVID-19 cases recorded during October 17 – November 26, 2000. Each data point represents a CSA. The larger the circle, the higher proportion of at-risk multi-generational households in the community.

The linear relationship in the figure is striking. It tells us that those communities recording the most new cases at the start of the recent surge continue to serve as foci of new COVID-19 cases as the surge continues. And the fact that the data points at the upper right are the fattest, while those at the lower left are the skinniest, confirms that CSAs with lots of multi-generational households continue to drive the epidemic.
Figure 5 below displays an updated version of the graphs that we showed in our October 17 and November 28 posts. The graph relates the recent incidence of COVID-19 infection on the vertical axis to the prevalence of at-risk households across some 300 CSAs in Los Angeles County, as measured on the horizontal axis. The graph tells us that a 10-percentage point increase in the prevalence of at-risk households is associated with a 51-percent increase in COVID-19 diagnoses. This relationship has not let up since the days of Phase II, when the epidemic began to concentrate in specific communities.

These findings for Los Angeles County should come as no surprise. The importance of inter-generational transmission has been established specifically in Florida’s most populous counties, and in the US and EU generally.
