A Non-Linear Tale of Two Counties

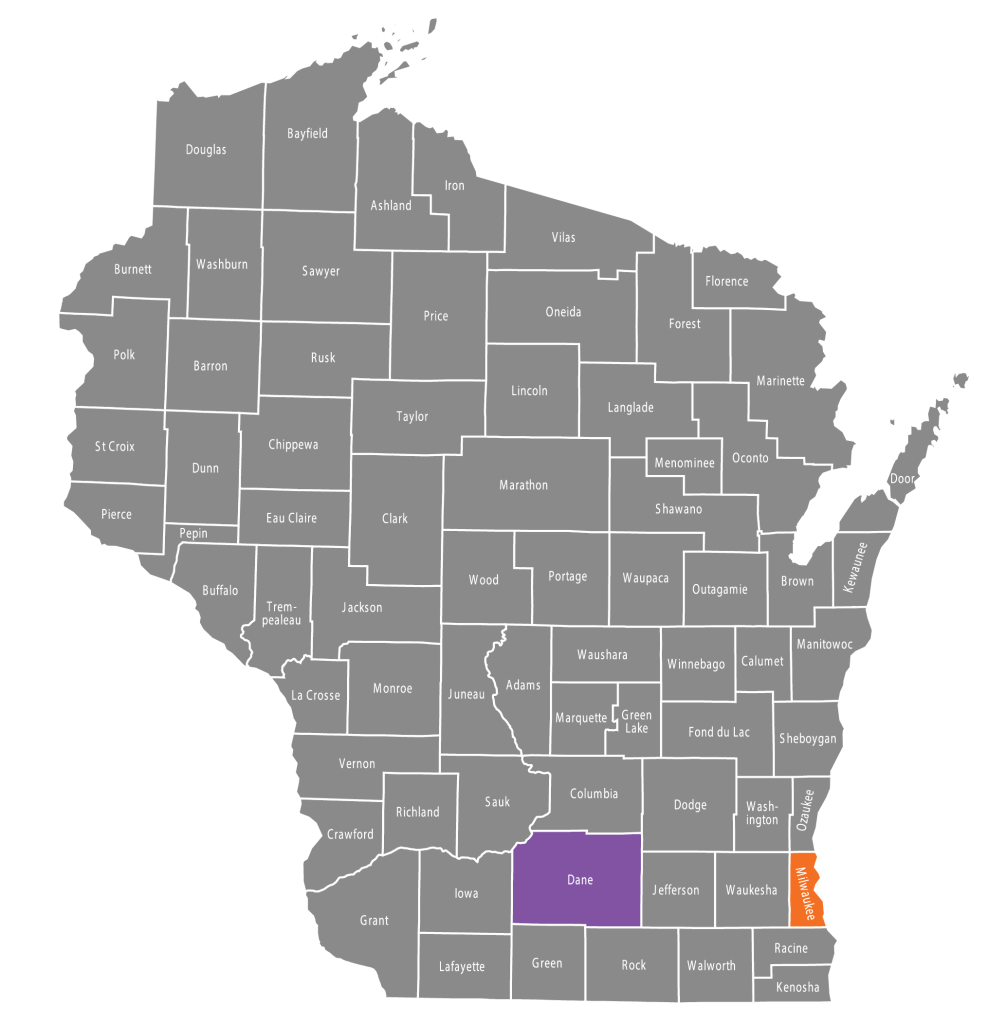
We begin with a comparison of the incidence of confirmed daily COVID-19 cases in Wisconsin’s two most populous counties: Milwaukee County, which includes the City of Milwaukee; and Dane County, which includes the City of Madison. Raw counts of positive COVID-19 cases in these two counties are regularly reported by the Wisconsin Department of Health Services. We rely here on the data posted on July 23, 2020. In the graphic above, we have converted the raw case counts into daily incidence rates per 100,000 population, based on 2019 populations of 945,726 for Milwaukee County and 546,695 for Dane County. The orange-colored points are the Milwaukee County data, while the purple-colored points are the Dane County data. As in earlier articles, we have plotted the incidence rates on a logarithmic scale, shown at the left. That way, a straight line in the graph corresponds to exponential epidemic growth.
The two counties are situated in the same state. They share the same governor, the same state legislature, the same state supreme court, and the same state department of health. They have been subject to the same statewide policies. Yet they show distinct patterns of evolution of COVID-19 cases during nearly five months that the United States has endured the pandemic. Our task here is to inquire why.
No Excuses
What is so striking about the above graphic is the strange interlude between the end of March and the end of June when the Dane County data points drop an order of magnitude below the Milwaukee County data points – almost as if a purple cable had come loose from its orange trestle. One could argue that these divergent trends are simply meaningless noise, inasmuch as counts of confirmed COVID-19 cases are thought to vastly understate the actual number of infections. But there’s a limit to how much one can rely on this pat excuse for dodging what appears to be genuine evidence.
The March 24 Safer at Home Order
Like many populous areas in the United States, coronavirus infections in Milwaukee and Dane Counties were surging in early March 2020. The two counties’ incidence curves began to flatten only after Secretary-Designee of Health Services Andrea Palm issued her Safer At Home Order on March 24, which kept non-essential businesses closed throughout the state for an entire month. For some reason, however, the statewide wide order had a much more pronounced effect in Dane County, bending the epidemic curve downward, while in Milwaukee County, there was at best a flattening of the curve.

The April 7 Primary Elections
One possible explanation for the initial divergence of the two epidemic curves is the differential response of the two counties to the statewide primary elections. In an attempt to minimize in-person turnout at the polls, Gov. Tony Evers on March 27 called on the legislature to send an absentee ballot to every voter in Wisconsin. When the legislature rejected the proposal, the governor issued an executive order postponing in-person voting in the election for two months. That order, however,was blocked by the Wisconsin Supreme Court, and the spring primary elections went forward on April 7, as marked in the graphic below.

The severe shortage of poll workers on primary election day had a much greater impact on the density of voting in Milwaukee County than in Dane County. To accommodate the shortage, only 22 percent of Milwaukee County voting locations were allowed to open, compared to 78 percent of Dane County locations. The consolidation was even more severe within the city of Milwaukee, where 325 polling sites were collapsed into just five. According to one press report, voters in some Milwaukee precincts had to wait in line up to 2 1/2 hours to cast their ballots. “Now, over two weeks later,” wrote the newly elected justice to the Wisconsin Supreme Court in a follow-up opinion piece, “we have an uptick in Covid-19 cases, especially in dense urban centers like Milwaukee and Waukesha, where few polling places were open and citizens were forced to stand in long lines to cast a ballot.”
The hypothesis that the long lines at Milwaukee’s primary polling places served as a seed for an upswing in COVID-19 cases has been subject to more than passing investigation. In a case tracking study, the Milwaukee County COVID-19 Epidemiology Intel Team identified numerous individuals who were diagnosed as COVID-19 positive during the three weeks after the primary election, but the team could not reach any definitive conclusions from the interview evidence alone. An econometric study of Wisconsin counties found that the proportion of cases testing positive in the three weeks after the primary was directly related to the number of in-person voters and inversely related to the number of absentee voters.
We’re left with the disturbing fact that Dane County, which felt little impact from the consolidation of polling places, continued to flatten its epidemic curve during the three weeks after the primary. Meanwhile, Milwaukee County’s epidemic curve began to reverse itself one week after the election. As we noted in San Antonio Conundrum, the timing fits with the evidence on the 5-day incubation of the disease. What’s more, the serial interval between the time the infector gets sick and the time the infectee gets sick is only about 5 or 6 days. That would give enough time for people infected at the primary to transmit the virus to others.
The Wisconsin Supreme Court Intervenes Again
On April 20, Gov. Evers announced his Badger Bounce Back plan to gradually reopen the Wisconsin economy. Adhering to the recent White House guidelines for Opening Up America Again, Evers’ plan continued the state’s Safer At Home restrictions, requiring that non-essential businesses remain closed until there was a sustained 14-day decline in COVID-19 cases. Golf courses, however, were allowed open, and exterior lawn care was permitted. A week later, Secretary-Designee Palm announced an Interim Order to Turn the Dial, allowing non-essential businesses to make curbside drop-offs and opening up outdoor recreational rentals and self-service car washes, so long as social distancing measures remained in place.
The governor’s carefully crafted regulatory scheme, however, would not stay in place for long. On May 13, upon petition of the legislature, the Wisconsin Supreme Court ruled that Palm’s Safer at Home order did not adhere to established rule-making procedures and was therefore unenforceable. While Palm indeed had some power to act in the face of the pandemic, her order to confine people to their homes and close non-essential businesses exceeded her authority.

Madison & Dane County Respond
With the court’s nullification of the statewide Safer at Home order, Wisconsin’s public health policy toward the COVID-19 epidemic devolved into a collection of variegated, asynchronous, substitute measures taken at the county and municipal level.
On the same day as the Supreme Court order, Janel Heinrich, Public Health Officer for Madison and Dane County, issued her own order adopting essentially all of the governor’s regulatory scheme – Safer at Home, Badger Bounces Back, and the Interim Order to Turn the Dial – but with reduced restrictions on religious entities. “Data and science will guide our decision making,” announced Madison Mayor Satya Rhodes-Conway. Five days later, the county set in motion its own Forward Dane Plan, which implemented a cascade of emergency orders – on May 18, May 22, June 5, June 12, and June 25, gradually loosening restrictions on social distancing. The May 22 order, in particular, allowed the opening of businesses, including salons, indoor restaurant and bar operations, to 25 percent capacity. The June 12 order increased the allowable threshold to 50 percent capacity.
The July 1 order, however, took a very different position. COVID-19 incidence had been rising in Dane County since the week after the Wisconsin Supreme Court nullified the statewide plan. “An emerging pattern in Dane County confirms that bars and mass gatherings create particularly challenging environments for the COVID-19 pandemic,” the order’s preamble noted. With the new order, indoor seating in restaurants was cut back to 25 percent of capacity. Bars – which technically entailed any business earning more than half of its revenues from alcoholic beverages – were again restricted to pickup and takeout. The most recent July 7 order required the wearing of a face covering while taking public transportation, waiting in line, and remaining indoors with non-family members.
City of Milwaukee & Milwaukee County Suburbs Respond
When it came to public health, the City of Madison and Dane County operated essentially as a unified entity. But that was hardly the case in Milwaukee County.
Back on March 25, City of Milwaukee Commissioner of Health Jean Kowalik had already issued her own stay-at-home order that pretty much paralleled Safer At Home. So, when the Wisconsin Supreme Court decision came down on May 13, Commissioner Kowalik initially elected to keep the existing local order in place. That apparently did not sit well with the 18 suburban communities constituting the rest of Milwaukee County, who issued their own new order. Starting May 22, according to their new Phase A/B/C/D plan, restaurants and bars could reopen with a recommended capacity of 50 percent, while salons and gyms could open up with a recommended 25 percent capacity. The very next day, the city’s Mayor Tom Barrett, aligning himself more closely with the suburban Milwaukee communities, decided to issue his own Moving Milwaukee Forward order allowing salons and playgrounds to reopen.
From that point onward, the City of Milwaukee adhered to its own phase 1/2/3 plan, while the suburban Milwaukee communities continued to follow their phase A/B/C/D plan. On June 12, the communities entered into Phase C, allowing mass gatherings of up to 50 persons and relaxing capacity constraints for restaurants and bars to 75 percent and gyms to 50 percent. But with COVID-19 case counts on the rise in early July, the communities held back on scheduled Phase D, which would have reopened restaurants, bars, salons and gyms to full capacity. Meanwhile, the City of Milwaukee moved forward with its Phase 4, allowing retail stores, restaurants and bars to open at 50 percent. Salons were to be held to a capacity of one customer per stylist, while faith-based gatherings and gyms were restricted to the lesser of 50 percent capacity or one person every 30 square feet.
By July 13, with COVID-19 counts continuing to rise both in the city and suburbs, the Milwaukee Common Council adopted the Milwaukee Cares Mask Ordinance.
The Bars
There is simply no way we can assign each blip and dip of the COVID-19 incidence curve to a particular event along the timeline of successive regulatory actions taken by the two counties. We need an overarching theme – a common underlying mechanism – to bring all the facts together. To that goal we now turn.

The graphic above displays the daily indices of visits to bars located in Milwaukee and Dane Counties during March 1 – June 30, 2020. The graphic is derived from the Patterns database maintained by SafeGraph, which we have already used in San Antonio Conundrum and TETRIS for Tulsa. The database follows the movements of a cohort of smart phone users who have consented to leave their location trackers activated. For every day from February 17 through June 30, we computed the number of entries into each of 240 Milwaukee County bars and 230 Dane County bars. We selected bars first on the basis of the business name, including Bar, Tap, Tavern, Pub, Lounge, Speakeasy, Cocktail, Ale, Saloon, and Brew. We then added specific businesses in each county based on lists of bars maintained by Yelp. To make the two series compatible, we normalized the numbers of entries so that the mean for the period February 17 – March 13 was equal to 100.
After entries into bars plummeted in March, there was a persistent difference in the volume of visits between Milwaukee and Dane counties. For example, during the week starting Monday, April 6, the geometric mean values for the two indices were 27 for Milwaukee County and 17 for Dane County. By mid May, the indices had begun to rise for both counties, but more rapidly for Dane County. By the week starting Monday, June 8, the indices were 53 for Milwaukee and 52 for Dane, respectively – in other words, about half of pre-epidemic activity levels.
While it is difficult to line up the dates precisely, the gap between the two counties in the index of visits to bars tracks the corresponding gap in the COVID-19 incidence. To interpret the relationship between the two graphs, one needs to understand that the two measured phenomena involve very different time constants. The number of visits to a bar on a given day can abruptly turn on a dime. The resulting change in COVID-19 incidence will take at least two weeks to play out, and even longer when one considers secondary spread.
How Non-Linearity Works
In early April – even before the spring primary election – the bar-entry indices averaged 27 for Milwaukee County and 17 for Dane County. That’s a ratio of 27/17 = 1.6. Yet at the same time, COVID-19 incidence in Milwaukee County was already about 6 times that in Dane County. The magnitudes, it would seem, don’t line up.
But they do. And the reason is the inherent non-linearity in the relationship between social distancing indices and disease transmission outcomes.

The graphic here displays a computer simulation that addresses this question. Each square represents an enclosed space – it could be a bar room, but it doesn’t have to be – in which a specified number of patrons are randomly and uniformly distributed. On the left, there are 17 patrons, each represented by a solid purple dot. On the right, there are 27 patrons. The first 17 patrons, colored purple, are in exactly the same locations as their counterparts on the left. The additional 10 patrons have been colored in orange to distinguish them. The left and right panels are intended to capture the differences in density between a Dane County bar and a Milwaukee County bar in early April. Strictly speaking, the density within the bar room at any point in time is not necessarily equal to the flow of patrons into the bar, as gauged by our social mobility indices above. But at least it’s a start at capturing the idea.
Surrounding each patron is a gray circle with the same radius. Focusing sharply on the droplet mode of transition, we are trying to capture the maximum distance between an infector and infectee patron. Transmission occurs only if one of the patrons is inside the radius of the other.
Let’s see what happens as the number of patrons increases. On the left, with 17 patrons, patrons A and B are just within each other’s radius. Everyone else is too far apart to get infected. Now move to the right, where there are 10 new patrons. C and D are paired – C was there from the start and D has entered the bar room and C’s radius. But that’s just one new pairing. Altogether, a total of 12 patrons are now at risk of transmitting and receiving an infection. That’s a six-fold increase in transmission risk for a 60-percent increase in capacity.
We hope the point is clear. Epidemic containment could be going along just fine at a capacity limit of (say) 25 percent. What might appear to be an incremental relaxation to (say) 50 percent could be an invitation to disaster.
Why This Is Really Important
The non-linearity arises here from the fact that the risk of transmission from one person to another falls off abruptly when the two are separated by a distance exceeding the size of infected person’s contaminated droplet cloud. That is the critical mechanism that permits us to explain why strict social separation initially works, but then fails to contain the spread of coronavirus as the relaxation of distancing measures proceeds.
One might counter that the index of bar visits is interesting but wildly over-interpreted. After all, during the initial Safer At Home phase, the bars were closed to all service but pickup and takeout. We wonder how well those restrictions were enforced, especially in a world where a bar with a food menu can at least maintain the pretense that less than half its revenues are from alcoholic beverages. In any event, we need to think of the index of bar visits as an overall indicator of the extent of social distancing. We are not asserting that all or even most coronavirus transmission occurs in that venue.
When we studied the sixteen most populous counties in Florida, we found that incidence trends ran pretty much in parallel. COVID-19 cases fell together and then rose together. Younger persons came down with the virus first, and then they gave it to socially less mobile older persons. Here, we have a unique opportunity to study a divergence in trends between two counties whose major urban centers are only about 80 miles apart. We have confirmed that a social distancing indicator still holds up as the key intermediate variable in explaining the widening and narrowing of the epidemic gap between the two counties.
We cannot broadly conclude that the Wisconsin Supreme Court decision on May 13 to nullify the statewide Safer At Home order was the but-for cause of the COVID-19 rebound in Madison and Dade Counties. For we do not know what social distancing measures would have prevailed in a counterfactual world with Safer At Home still in place. But we can more narrowly conclude that the Court’s decision triggered the replacement of Safer At Home with a motley collection of uncoordinated, asynchronous local measures that ultimately opened the door to a debacle.
Acknowledgments: Thanks to Prof. Chad Cotti for supplying the data on the consolidation of polling locations in Milwaukee and Dane Counties during the April 7, 2020 primary elections.
Addendum: Prof. Martin Andersen and Dr. Paul Cieslak have both drawn attention to the dismissal of approximately 7,800 University of Wisconsin students who were living in dormitories at the start of spring break on March 14. Could this massive exodus alone have accounted for the substantial divergence in COVID-19 incidence rates between Dane and Milwaukee Counties ? Yes. But only under the extreme assumption that the dismissal staved off a major outbreak of 50 cases in the dorms. That would come to a rate of 640 per 100,000 students, comparable to that seen among front-line Metropolitan Transit Authority workers in New York City during March and April.
Addendum: In the computer simulation above, we focused on the number of patrons who were located within the infectious radius of at least one other patron. Prof. Dan Spielman has suggested a better indicator of overall transmission risk, in particular, the number of pairs of individuals within the infectious radius. After all, patron M in the bar room with 27 patrons (at the right above) is at higher risk than the others because she’s in three distinct pairs with patrons K, L, and N. Prof. Spielman’s approach leads to a general formula that applies to any bar room, including a rectangle, an ell, or an oval. For a particular shaped room, let 





Addendum: This article has been accepted for publication in Research in International Business and Finance.