We went back and looked at COVID-19 incidence and bar attendance in Dane and Milwaukee counties.
A lot has happened in the state of Wisconsin since we last reviewed its struggles with the continuing COVID-19 epidemic. (Our last review was subsequently published here.)
On October 6, Wisconsin Department of Health Services Secretary-designee Andrea Palm issued Emergency Order #3, restricting indoor gatherings in stores, restaurants, bars and other public venues to 25-percent capacity. “The State of Wisconsin is in the midst of a deadly, uncontrolled, and exponentially growing spike in cases of COVID-19,” noted the order’s preamble. “Some Wisconsin hospitals are already struggling to keep up with care demands – both because of bed space and staffing shortages – and we have to do what we can to slow down the spread of this disease so our health care workers can keep up,” noted the accompanying FAQ. Five days later, on October 11, the weekly state report of the White House Task Force declared, “Wisconsin has seen a sustained peak of epidemic activity in the last week with an ongoing health emergency.”
The following day, St. Croix County Circuit Judge R. Michael Waterman upheld Gov. Tony Evers’ August 1 emergency order mandating the use of masks in enclosed public spaces. At least for the moment, it looked like the state government was finally recovering from the aftermath of the Wisconsin Supreme Court’s decision back on May 13 to nullify Secretary Palm’s original statewide safer-at-home order of March 24.
But then on October 14, Sawyer County Circuit Judge John Yackel temporarily blocked Secretary Palm’s October 6 order limiting the indoor capacity of stores, bars and restaurants. That same day, the state opened a field hospital in State Fair Park as the census of hospitalized COVID-19 patients crossed the 1,000 threshold. On Monday, October 19, Secretary Palm was to appear in court to defend her order.
COVID-19 Incidence in Dane and Milwaukee Counties
Figure 1 below shows the daily incidence of newly confirmed COVID-19 cases in Wisconsin’s two most populous counties from March 15 through October 16. When we last took a snapshot on July 24, the incidence of new cases was starting to come back down in the wake of a July 7 local order requiring the use of face masks while taking public transportation in the city of Madison and the rest of Dane County, as well the July 13 adoption by the Milwaukee City Council of the Milwaukee Cares Mask Ordinance.

From the first week of August onward, however, new COVID-19 cases resumed their upward climb. We’re still investigating whether the apparent bump in Dane County cases (purple data points) in early September can be wholly attributed to an outbreak at the University of Wisconsin in Madison. Still, the point is clear, the local mask-related orders of July had at best a temporary effect.
Bar Attendance in Dane and Milwaukee Counties
Figure 2 below shows the daily trends in bar attendance in the two counties through September 30. The graphic is derived from the Patterns database maintained by SafeGraph, which we’ve previously used to study gym attendance in Los Angeles County since February 2020, restaurant attendance in San Antonio around the time of street protests during May 30 – June 11, 2020, and visitors to President Trump’s rally in Tulsa on June 20, 2020.

The database records the movements of holders of smartphones with location-tracking software. For every day from February 17 through September 30, we computed the number of entries into each of 240 Milwaukee County bars and 230 Dane County bars. To make the two series compatible, we normalized the numbers of entries so that the mean for the period February 17 – March 13 was equal to 100. The figure shows the normalized series from March 1 onward.
When we last looked at the bar-attendance data, the gap in attendance between the two counties from mid-March through the end of May had already disappeared, and the number of visits in both counties was hovering around 60 percent of its pre-epidemic baseline. Since then, bar visitation has risen to around 70 percent of baseline, with attendance on some weekends exceeding 90 percent.
What Happened?
The temptation here is simply to assign all the blame to the bars. A fairer interpretation is that the bar-attendance data are no more than an indicator of a broader pattern of increasing social activity in the face of repeated governmental efforts to promote mask wearing and reduce crowding in public venues. At least in the two most populous counties in Wisconsin, the data suggest that these governmental efforts have had only limited, temporary effectiveness, with their impact repeatedly wearing off in a matter of weeks.
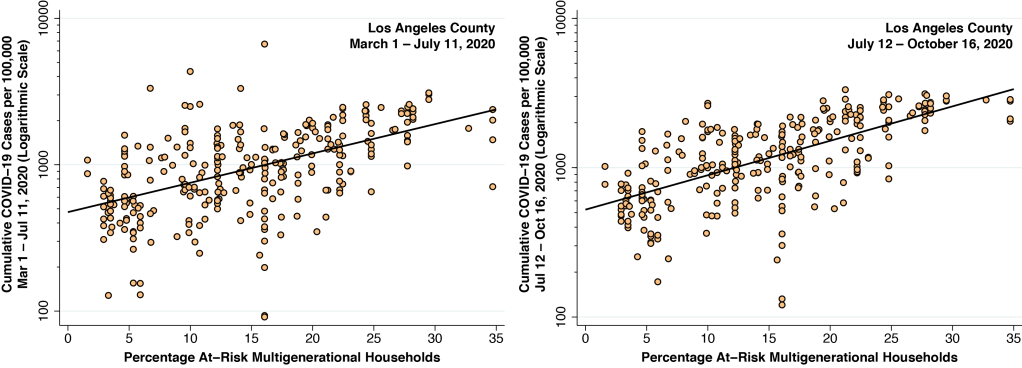
At the peak of the COVID-19 epidemic in Los Angeles County during the first half of July, newly confirmed COVID-19 diagnosis were running at about 210 per 100,000 population per week. Since then, the incidence rate has dropped to about 70 per 100,000 per week. But for the high prevalence of multi-generational families at risk for intra-household transmission, we’ve maintained that the COVID-19 incidence rate in Los Angeles would now be much lower. In Wisconsin, by contrast, the most recent data are running in the range of 225 confirmed cases per 100,000 per week in Dane County and 300 per 100,000 per week in Milwaukee County.
One explanation is that there is so little political consensus in Wisconsin that state and local governments are effectively paralyzed, or at least severely constrained into taking half-measures. Another is that governmental orders to wear masks and stay out of bars are effective only if accompanied by compelling messages. Admonitions to protect yourself or to protect others, we’ve maintained, need to be replaced by messages to protect your family. In any case, our research needs to stop asking whether public policies work and start inquiring when and where they work.