Death rates have fallen in Florida in all age groups over 50 years old. Is it because we’ve developed new treatments, or because we’ve learned what not to do?
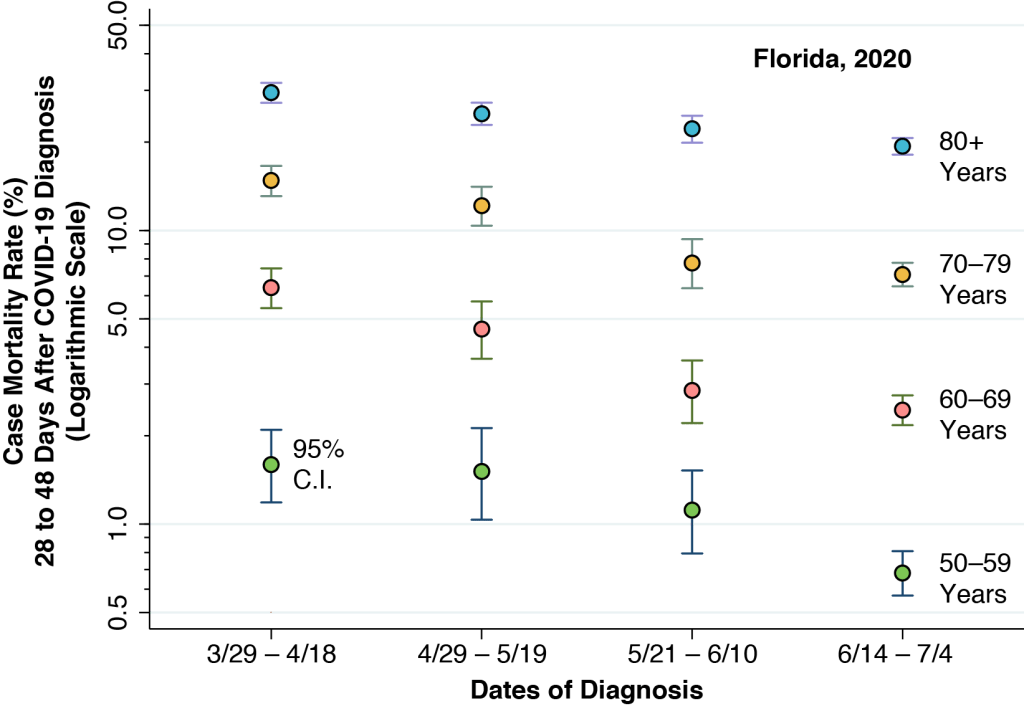
The graphic above shows the case mortality rate among persons diagnosed with COVID-19 in Florida during four successive time periods, as indicated along the horizontal axis. During each time period, individuals were followed for at least 28 days after their initial diagnosis in order to ascertain their vital status. The individuals are grouped above by age: those 50-59 years old denoted by lime-colored points; those 60–69 by pink points; those 70–79 by mango points; and those 80 years or more by cyan points. We calculated the case mortality rates from data released by the Florida Department of Public Health, as described in this technical report. We previously used the same data source to study the propagation of the disease from younger to older persons after the reopening of the state in mid-May.
The graphic shows significant declines in case mortality in all four age groups. With the exception of the transition from the first diagnostic interval to second in the case of 50- to 59-year-olds, the changes have been continuous from one interval to the next.
Not Entirely a Novel Observation
The observation that case mortality rates have been headed downward is not entirely novel. Declining in-hospital mortality from COVID-19 pneumonia was reported in San Raffaele Hospital in Milan, Italy during February 25 – May 20. Similarly declining in-hospital mortality was reported in Colorado hospitals during March 1 – May 31, and in United Kingdom hospitals during March 24 – June 14 and critical care units during March 1 – May 30. Declining case mortality has also been mentioned in the local press in Hawaii, Louisiana, and Illinois.
So what, if anything, makes the current study distinctive? For one thing, it kept track of hospitalized COVID-19 patients even after they’ve left the hospital. It also kept track of COVID-19 victims who were never hospitalized to begin with. What’s more, it kept track of everyone for a specified follow-up interval of at least 28 days – long enough to find out if the patient died.
Is the Drop in Mortality No More Than an Illusion?
While the current study may have made some methodological advances, that’s not the main question here. Declining case mortality has now been reported with sufficient regularity to pose a more difficult question: Is the observed drop in mortality real?
Let’s dispose of the first possibility – namely, that the apparent mortality decline is a statistical illusion resulting from inadequate tracking of COVID-19 fatalities. Prior studies of in-hospital mortality, one might contend, have been missing deaths that occurred after hospital discharge. Grandpa was sent home at the end of week 2 when his blood oxygen saturation came back up, and then he died suddenly at home during week 3 of a massive blot clot in his lung. The current study obviates this potential bias by tracking patients in and out of the hospital and for long enough to capture the life-threatening blot clots that have been observed later in the course of the acute illness. One might contend instead that Florida has been losing track of nonresidents whose death certificates went to vital records departments in other states, but there just aren’t enough of these out-of-state patients to bias the mortality rates significantly.
The second argument that the apparent mortality drop is illusory is far more slippery and imprecisely framed. Increasingly mild cases of SARS-CoV-2 infection, so the argument goes, have been picked up as a result of expanded testing. These additional milder infections have diluted the overall pool of COVID-19 cases and thus artificially lowered the death rate. In view of the observed declines in mortality seen above in every age group over 50 years, this alternative explanation would require us to posit that the expanded testing has identified ever milder cases among 80-year-olds. In view of the multiple studies documenting declines in mortality among hospitalized patients, we would be further required to posit that doctors have been admitting ever milder cases to the hospital. As we’ll see below, there is evidence that just the opposite trend has been occurring.
What’s more, the available evidence strongly contradicts the hypothesis that expanded testing has been pulling less severe cases into the state’s COVID-19 registry. To the contrary, increased disease incidence has been pushing up the demand for testing. (See Florida: Coronavirus Infections Push Tests, Testing Does Not Pull Infections.)
Finally, one needs to inquire whether there is really any concrete evidence in favor of the dilution hypothesis. The standard PCR test to determine whether a nasal or throat swab has coronavirus RNA actually reports a numerical index called the cycle threshold or CT. The lower the CT, the more virus the patient harbors. We haven’t seen any reports that the average CT value of the typical coronavirus-positive sample has been creeping up. Or that fewer infected patients have a blood oxygen saturation below 95 percent. The best we can do is speculate that there may be persons out there with sufficient cross-immunity from other coronaviruses to attenuate a SARS-CoV-2 infection without blocking the infection altogether, and that these individuals are now getting detected in substantial numbers.
Learning by Doing
We’re left with the conclusion that the decline in case mortality is, in all likelihood, real. And that leads us to an even more difficult question: How did it happen?
Our contention here is that the observed improvement is COVID-19 case survival is the result of the accumulation of a significant number of incremental improvements in patient care learned on the job – what economists have long called learning by doing.
At the risk of over-explaining the basic point, we’ll head to the kitchen. Let’s say you’re trying make clafoutis, a French dessert with fruit and a custard-like creamy filling. If you bake it too little, the dessert is runny and tastes like eggs. If you bake it too much, your guests won’t appreciate the chalky custard. You’ve got to make clafoutis several times to really get the hang of it. To take a more complex example, once an organ transplant team has worked together on hundreds of cases, the transplant surgery goes faster, there are fewer complications, and the organ recipient’s long-term survival is improved.
A natural response to the learning-by-doing hypothesis is that it’s no big deal or, even more stinging, it’s completely obvious. After all, the press has been reporting for months that doctors have found alternatives to ventilators for serious ill patients, have discovered how positioning patients in the prone position improves breathing, and have learned that blood thinners can stave off a fatal stroke or a massive blood clot in the lung.
But there’s more going on here. Informal advances in the clinical care of COVID-19 patients, very often encountered through trial and error, motivated the randomized controlled trials that ultimately established new standards of treatment. Not the other way around. The idea that the common steroid dexamethasone could check disastrous inflammation was in the air well before a formal study demonstrated its life-saving benefits. Doctors were battling to get the antiviral drug remdesevir well before federal regulators gave the green light to its widespread use.
Enhanced Productivity
When we talk about learning by doing, we’re not necessarily referring to advances embodied in a particular clinical technique or therapeutic intervention. Sometimes, workers simply get better at their jobs without adopting any new, distinct technology. The press is filled with vignettes about how these doctors have learned to do this and those doctors have learned to do that. In fact, it is the entire healthcare team that has learned how to work better.
In the case of improvements in COVID-19 care in seriously ill patients, we’ll venture an educated guess that the most increasingly productive members of the healthcare team have been the intensive care unit nurses. It was the ICU nurses, we contend, who made the extraordinary discovery that the oxygen level of a COVID-19 patient can rapidly deteriorate without the patient looking short of breath. That’s because the lungs somehow maintain the natural compliance that lets the chest move up and down with each breath, even while the tiny air sacs responsible for exchanging oxygen are flooded with inflammatory liquid.
Learning What Not To Do
One of the most critical ways that learning by doing can advance clinical care is by figuring out what doesn’t work. This is not the place – Or is it? – to enumerate all the blind alleys we’ve had to pull back from. We hope that outpatient providers have stopped administering nebulizer treatments that spread coronavirus-laden aerosol into the lungs of other as-yet uninfected patients. We hope that ICUs have opted for non-invasive ventilation when trained respiratory technicians were unavailable to properly operate ventilators.
We know that hydroxychloroquine prescriptions in U.S. pharmacies surged through March 2020. But we have not seen data on the medication’s subsequent use once specialty societies began to caution that its attendant risk of cardiac complications was substantially enhanced in COVID-19 patients, if only because the virus appeared to attack the heart directly. We wonder, with good reason, whether the observed improvement in case mortality was attributable in part to widespread learning that hydroxychloroquine was not the drug to prescribe.
Not Just in the ICU
Lest any reader assume that the improvements in care were exclusively an accomplishment of the hospital team, we point to the growing volume of patients who are discharged to home on portable oxygen tanks, many of whom learned to give themselves subcutaneous injections with blood thinners. Those nurses who taught those patients how to inject themselves – and the interpreters who translated their instructions into fourth-grade vocabulary in the patient’s native language – saved their lives. The technicians who transported and set up the oxygen tanks in their bedrooms saved their lives. The primary care physicians, nurse practitioners and physicians assistants who on the front line identified the sickest patients and got them to the hospital just in time saved their lives. Without the blare of trumpets or the roll of drums.
When Not to Go to the Hospital
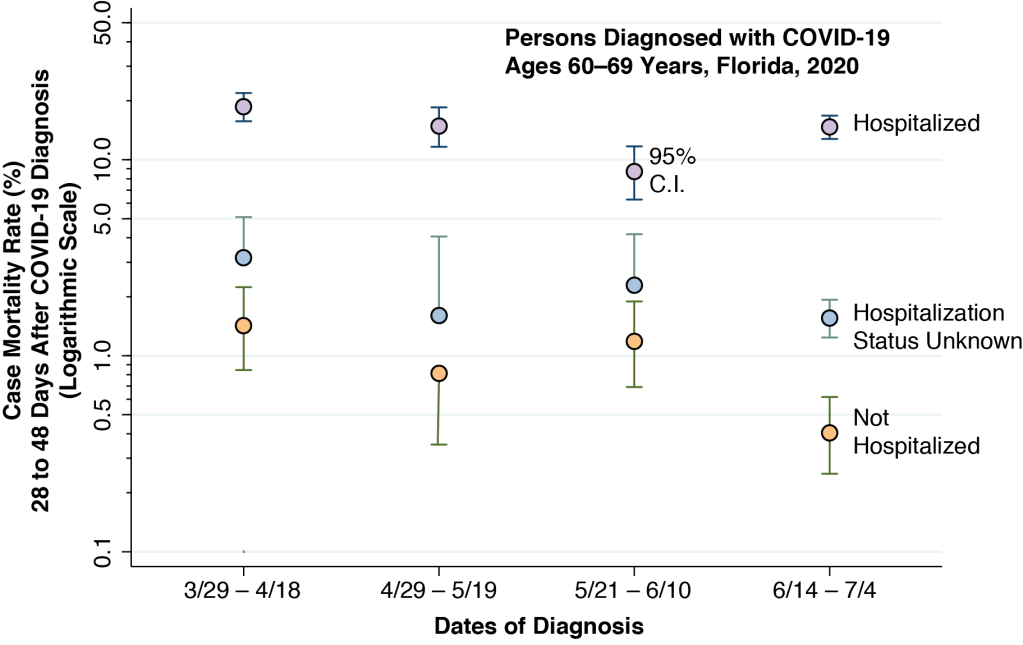
The Florida Department of Public Health also collected information on the hospitalization status of every person diagnosed with COVID-19. Unfortunately, delays in ascertaining whether someone was hospitalized limit the reliability of this source of information. Still, we can learn something from the results for persons aged 60–69 years old, as indicated in the graphic above.
For each of the four diagnostic intervals, the graphic shows the case mortality rate for 60- to 69-year-olds known to have been hospitalized (lilac points), those known not to have been hospitalized (peach points) and those with unknown hospitalization status (sky-blue points). Among those who were hospitalized, the mortality rate progressively declined during the first three intervals, but then increased in the fourth interval (6/14 – 7/4/20). Among the two other groups, the case mortality rate did not show a clear pattern during the first three intervals. During the fourth interval, the case mortality declined.
Among the 60- to 69-year-olds in the hospitalized group, the increase in case mortality raises the possibility of congestion effects. These adverse effects on the quality of care arise as a hospital nears capacity. As we wrote long ago, “There are queues in front of radiology. The supply of a certain type of blood is exhausted. The floor stock of chest tubes is out just as Dr. A declares Mr. X’s life-saving need for one. … As the degree of capacity utilization increases, previously stable risk-sharing arrangements break down. Doctors, fearing that they will not have access to the necessary inputs, grab up their own exclusive shares to keep themselves protected.”
There is, however, an alternative explanation for the data in the graphic. The marked decline in the case mortality during the fourth interval among those not hospitalized strongly suggests that many low-risk patients were no longer being hospitalized. Learning by doing, healthcare providers have come to understand more clearly who can be treated adequately outside the hospital.
This is not simply a passive transfer of cases from one data bucket to another. Under a wide range of circumstances, staying out of the hospital is good for your health. You’re less at risk for nosocomial infections. You remain more active at home, and thus can retain more muscle mass. You can eat home-cooked meals. You’re less depressed, less likely to end up sun-downing. And if your family can transfer you to a wheelchair, you can go out on the patio and see the clear night sky.
Commentary (Profa. Dra. Izabela Sobiech Pellegrini):
Prof. Pellegrini (Escola de Artes, Ciências e Humanidades – EACH|USP, University of Sao Paulo) reports comparable observations on declining case mortality among persons aged 50 years or more in the state of Sao Paolo, Brazil.

Commentary (Prof. Riccardo Puglisi):
