Nearly one in four hospital beds is now located in a hospital reporting a critical staffing shortage.
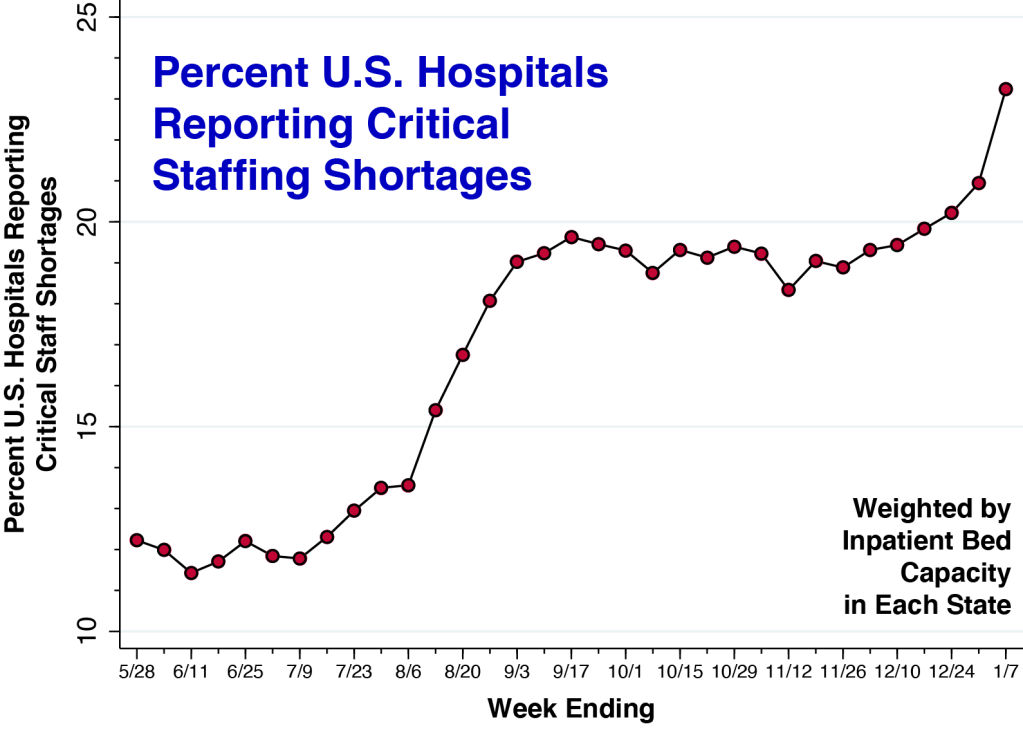
This post continues to update our earlier summary of trends in U.S. hospital staffing. During the Delta wave in the United States, the percentage of hospitals reporting critical staffing shortages rose from 12 to 19 percent. Even as hospital admission rates declined in October and November, the critical staffing percentage remained elevated at 19 percent. Over the past four weeks, as the Omicron variant has begun to spread, this percentage has increased to 23.2 percent.
To determine each data point in the figure, we first ascertained the percentage of hospitals in each state reporting a critical staffing shortage, as reported by the Department of Health and Human Services. We then computed the weighted average across all states, where the weights were each state’s inpatient bed capacity. During the week ending January 7, 2022, we’ve thus calculated that 23.2 percent of all U.S. hospital beds were located in a hospital reporting a critical staffing shortage.
Trends Vary Across States: New Mexico and Rhode Island
Trends in staffing shortages vary across states. Below we plot the percentage of hospitals with critical staffing shortages in two of the hardest hit states: New Mexico and Rhode Island.

The critical staffing shortage percentage in New Mexico has increased steadily from 24.9 during the week ending May 28 to 52.3 during the most recent reporting week ending January 7. By contrast, the proportion of Rhode Island hospitals with a critical staffing shortage shot up to about 50 percent with the emergence of the Delta wave in August and has remained at that level.
Vaccine Mandates are Unlikely to be the Primary Cause.
Some have contended that vaccine mandates are contributing to the emerging shortage of healthcare workers. But there is little concrete evidence to back up this contention. While a small minority of healthcare employees have chosen to leave their jobs, the vast majority have opted for vaccine protection. At large healthcare systems like Houston Methodist, Truman Medical Centers/University Health in Kansas City, the North Carolina hospital system, Advocate Aurora Health in Chicago, Mount Sinai Health System in New York, St. Claire Regional Medical Center in Kentucky, and Henry Ford Health System in Detroit, less than 1 percent of employees have had to be let go.
The Labor Market for Skilled Nursing Care was Already Tight.
Still others have pointed to the increasing fees charged by traveling nurses and nurse staffing agencies to compensate for growing vacancies among nurse employees. The plain fact, however, is that the tight labor market for hospital-based nursing care predated the COVID-19 pandemic. Annual turnover among hospital-based registered nurses was already up to 15.9% in 2019 and increased to 18.7% in 2020.
It’s All About Pandemic Burnout.
Far and away the most critical determinant of rising staff shortages has been burnout and peritraumatic stress among healthcare workers, with more nurses leaving their employment as the pandemic drags on. While burnout among frontline healthcare workers has always been a serious problem, the percent of surveyed hospitals reporting 10% or more vacancies for RNs abruptly rose from 23.7% in 2019 to 31.8% in 2020 to 35.8% by early 2021.
The evidence of burnout among frontline workers is overwhelming not only in the U.S., but many other healthcare systems, including China during the initial Wuhan outbreak. The president of the American Nurses Association recently asked the U.S. Secretary of Health and Human Services to declare a national nursing shortage crisis. A national strategy to address healthcare worker burnout as been repeatedly urged.
We’re talking about continuous exposure to traumatic stress from extended hours, time away from family, near-continuous use of personal protective equipment, fear of personally contracting COVID-19, loss of patients with whom workers have become emotionally attached, and the rising frequency of medical errors as emergency rooms and ICUs fill up. We’re talking not only about ordinary job burnout, but also compassion burnout.
The anti-vaccination movement is driven in part by conspiracy theories that sow doubt about the integrity of medical professionals. Has the resulting loss of confidence caused some healthcare workers to experience a disconnect from their beliefs in the value of their work?
Stay Tuned.
We will continue to follow the aggregate U.S. hospital staffing situation as the Omicron wave plays out.